

Skin tightening procedures usually mean choosing between downtime or disappointing results. RF microneedling devices like Morpheus8 changed that equation by delivering radiofrequency energy directly into the dermis through insulated microneedles—skipping the surface damage that comes with ablative treatments.
The technology combines mechanical injury with thermal remodeling. Tiny needles penetrate up to 4mm deep (compared to traditional microneedling’s 2-3mm maximum), and bipolar radiofrequency heats targeted tissue zones without cooking the epidermis. That depth matters for reaching subdermal fat and the reticular dermis where serious collagen remodeling happens.
The Science Behind Tissue Remodeling
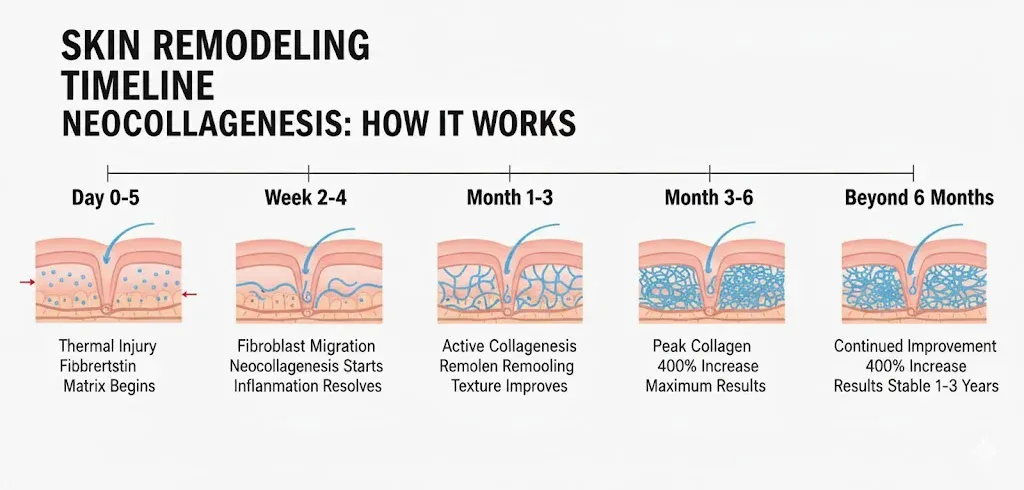
- Day 0-5: Thermal injury triggers fibroblast migration, fibronectin matrix formation begins
- Week 2-4: Neocollagenesis starts, early inflammatory phase resolves
- Month 1-3: Active collagen remodeling, visible texture improvements
- Month 3-6: Peak collagen deposition (400% increase documented), maximum clinical results
- Beyond 6 months: Continued improvement, results stable 1-3 years
The actual remodeling continues long after treatment. Neocollagenesis peaks around 3-6 months post-procedure. One histological study documented a 400% increase in collagen and elastin deposition at the 6-month mark after just four treatment sessions spaced monthly apart.
Unlike surface treatments that only penetrate the papillary dermis, the insulated needle design protects the epidermis while delivering energy precisely where structural changes occur. This explains why RF microneedling causes less post-inflammatory hyperpigmentation than CO2 lasers, making it viable for Fitzpatrick skin types IV-VI.
Clinical Results for Acne Scarring
Atrophic acne scars—the depressed kind left after inflammatory acne resolves—respond because RF microneedling targets the exact problem: insufficient dermal collagen supporting the epidermis above.
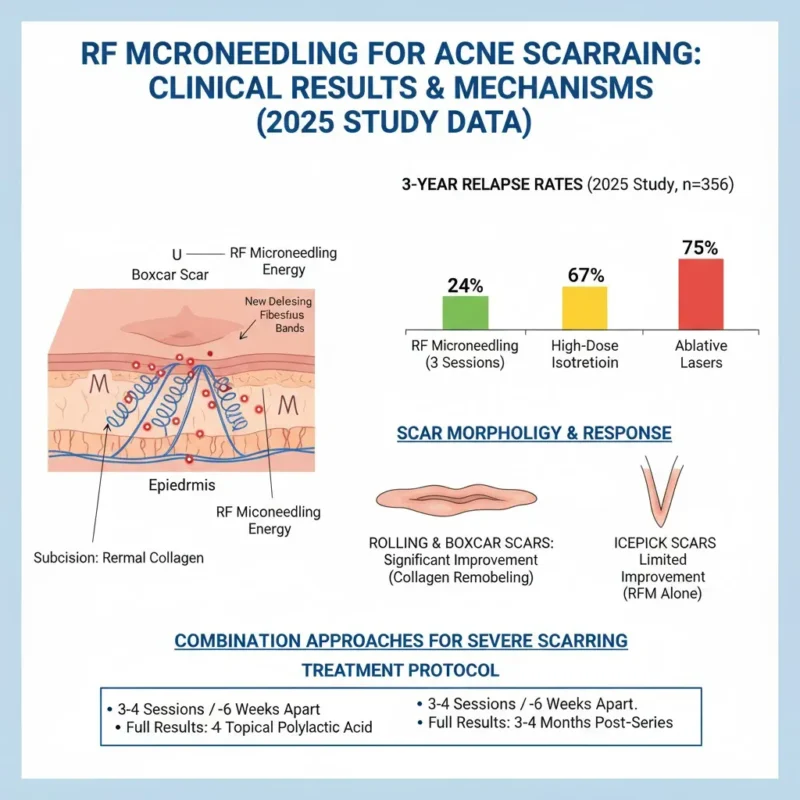
A 2025 study tracking 356 acne scar patients compared three modalities: high-dose isotretinoin therapy, ablative laser series, and fractional RF microneedling. The RF group received just three sessions. After three years of follow-up, relapse rates told the story: 24% for the RF microneedling group versus 67% for isotretinoin and 75% for ablative lasers.
Scar morphology determines response. Rolling scars (broad, M-shaped depressions) and boxcar scars (U-shaped with defined edges) improve significantly because the collagen remodeling gradually elevates the depressed tissue. Icepick scars—those narrow, V-shaped punctures extending deep into dermis—show limited improvement with RF microneedling alone.
For severe scarring, combination approaches work better. Studies pairing RF microneedling with subcision (releasing fibrous bands under scars) or topical polyactic acid showed superior outcomes compared to standalone treatments. The mechanical release combined with thermal remodeling addresses both tethering and volume loss.
Treatment protocols typically involve 3-4 sessions spaced 4-6 weeks apart. Some patients notice texture smoothing after the first session, but substantive scar filling takes the full series plus 3-4 months of collagen maturation afterward.
Skin Laxity and Tightening: The Numbers
Facial and neck laxity improves through two mechanisms working simultaneously. First, immediate collagen fiber contraction from thermal injury—think of it like heat-shrinking tissue. Second, the months-long neocollagenesis process that deposits fresh structural proteins.
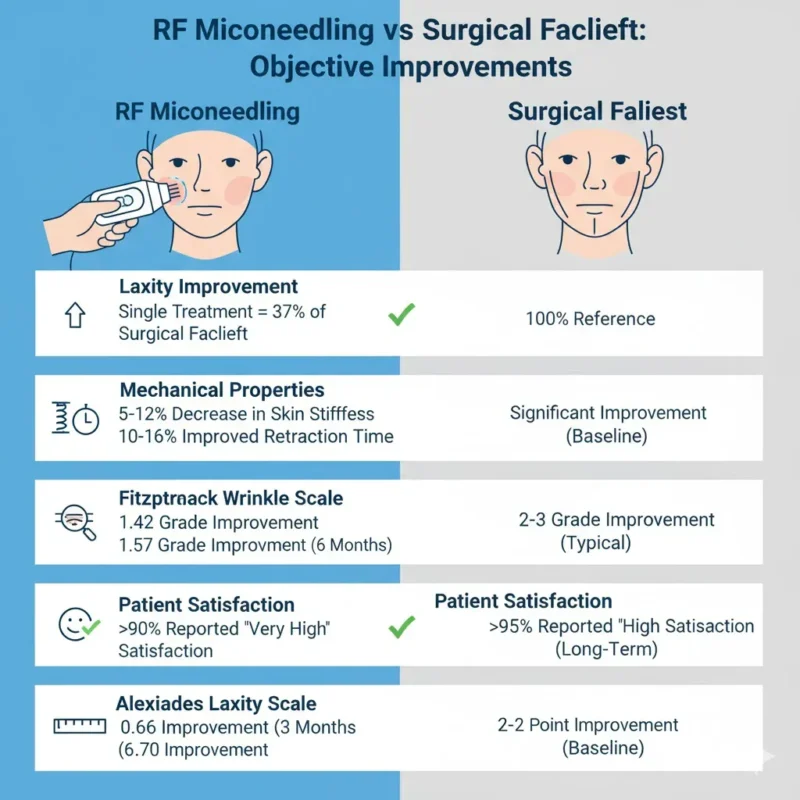
Interesting benchmark: the mean laxity improvement from a single fractional RF treatment measured 37% of what a surgical facelift achieves. Not replacing surgery, but closing a significant gap for patients between “do nothing” and “go under the knife.” Patient satisfaction hit >90% rating “very high” in multiple studies.
Body applications—arms, abdomen, thighs—require deeper penetration and often pair RF microneedling with bipolar RF devices that treat larger volumes of tissue simultaneously. The adjustable needle depth (up to 8mm on some devices) allows treatment of subdermal adipose tissue, not just skin.
A case study treating thigh laxity after significant weight loss used subcutaneous RF microneedling over two sessions. The Hexsel and Dal’Forno Severity Scale showed a 5-point improvement in cellulite appearance and skin tightness. The depth of depressions improved most, consistent with collagen deposition filling atrophic areas.
Stretch Marks: What the Data Shows
Striae distensae—stretch marks—are essentially dermal scars where collagen and elastin broke down from mechanical stretching. The atrophic, hypopigmented appearance of striae alba (old, white stretch marks) comes from reduced dermal thickness and melanocyte loss.
RF microneedling addresses the structural deficit. A prospective study treating stretch marks on abdomen, arms, thighs, and buttocks tracked 17 subjects through four treatment sessions at 4-week intervals. Using 3D photography analysis at 16 weeks post-final treatment:
- Average striae volume reduction: 19.1%
- Redness reduction: 14.3%
- Pigmentation improvement: 11.2%
- Overall color reduction: 8.82%
The Global Aesthetic Improvement Scale improved 1.7 points from baseline. Patients rated their satisfaction at 3.1 out of 4 (“satisfied”). Pain during treatment averaged 3.8 out of 10, tolerability scored 3.1 out of 4 (“tolerable”).
Multiple comparative studies pitted RF microneedling against fractional CO2 lasers for striae treatment. One Indian study found RF microneedling more effective with significantly lower post-inflammatory hyperpigmentation rates—critical for darker skin types where laser complications run higher.
Not all stretch marks respond equally. Fresh striae rubra (red/purple marks from recent stretching) improve more than mature striae alba. But even old stretch marks showed measurable volume reduction and texture smoothing. The controlled thermal injury stimulates collagen synthesis even in scarred tissue where normal remodeling stopped.
Recovery Timeline and What Actually Happens
Immediately post-treatment, expect the treatment area to look like moderate sunburn. Redness and mild swelling typically resolve within 1-5 days, though RF microneedling causes slightly more inflammation than traditional microneedling due to the thermal component.
The microscopic puncture wounds close fast. Most patients can apply makeup and sunscreen by day 2. Avoiding direct sun exposure for the first 48 hours isn’t optional—the thermal injury makes skin photosensitive temporarily.
Some dryness and flaking happens during week one as the superficial skin layer renews itself. That’s normal wound healing. The deeper dermal remodeling causing the actual clinical improvement operates on a months-long timeline that doesn’t produce visible peeling or downtime.
Early visible improvements appear around 4-6 weeks when inflammation resolves and initial collagen deposition begins. Peak results don’t show until 3-6 months post-treatment when neocollagenesis maxes out. This delayed gratification frustrates some patients expecting instant outcomes, but it’s inherent to how collagen synthesis works.
Results duration varies by area and individual factors. Facial treatments typically maintain improvement for 12-18 months before patients schedule touch-ups. Some body treatments hold for up to 3 years. Age, sun exposure, smoking, and skincare habits all impact longevity.
Who Shouldn’t Get This Treatment
Active skin infections anywhere in the treatment zone—acne breakouts, herpes simplex, impetigo—mean postponing treatment until resolved. Introducing microneedles through infected tissue spreads bacteria into deeper layers.
Patients with keloid-prone skin or active keloids need careful evaluation. While RF microneedling creates controlled micro-injuries rather than surgical incisions, any wound healing trigger can potentially cause keloid formation in susceptible individuals. Starting conservatively with test spots makes sense.
Recent isotretinoin (Accutane) use within 6-12 months is a relative contraindication. Retinoids affect wound healing and collagen remodeling. Most providers wait at least 6 months after discontinuing isotretinoin before performing RF microneedling.
Pregnancy and breastfeeding fall into the “wait until later” category—not because of proven harm, but because aesthetic procedures lack safety data in pregnant women. No compelling reason to take unnecessary risks.
The insulated needle design makes RF microneedling safer for darker skin types (Fitzpatrick IV-VI) compared to ablative lasers. The RF energy bypasses the epidermis where melanin could absorb energy and cause hyperpigmentation. Multiple studies confirm low PIH rates across skin types when proper settings are used.
Unrealistic expectations cause more problems than medical contraindications. Someone hoping to “erase” deep acne scars or eliminate severe laxity needs counseling about realistic outcomes. RF microneedling improves texture and produces measurable tightening, but it’s not a facelift alternative for advanced aging.
Comparing to Other Options
Traditional microneedling—using manual dermarollers or motorized pens—works through mechanical injury alone. Depth tops out around 2-3mm, and the remodeling response depends entirely on the needle punctures. Results lean toward surface texture improvement: fine lines, enlarged pores, mild scarring.
RF microneedling adds the thermal component that amplifies collagen synthesis and allows deeper tissue targeting. Studies show more dramatic improvements in fewer sessions compared to standard microneedling. The downside? Higher cost and slightly longer recovery.
Ablative lasers (CO2, erbium) vaporize epidermis and heat dermis—effective for wrinkles and scars but with longer downtime and higher PIH risk, especially in darker skin. RF microneedling trades some of that aggressive efficacy for better safety profile and faster recovery. Different tools for different situations.
Injectable treatments like fillers and biostimulators address volume loss through different mechanisms. Fillers provide immediate volume, biostimulators trigger gradual collagen growth. RF microneedling can’t replace lost volume but improves skin quality and tightness. Combination approaches often work better than choosing one modality.
Surgical facelifts remain the gold standard for severe laxity because they reposition tissue and remove excess skin—something energy-based devices can’t replicate. But surgery means incisions, anesthesia, recovery time, and permanent changes. The patient seeking moderate improvement without surgery finds RF microneedling fills that gap.
The treatment fits a specific niche: patients wanting more than topical treatments deliver but less than surgery requires. That middle zone where tissue quality needs improvement, laxity exists but isn’t severe, and scars or texture issues bother someone enough to try something beyond creams.
References
- Dermatologic facial applications of Morpheus8 fractional radiofrequency microneedling. PubMed, 2022. https://pubmed.ncbi.nlm.nih.gov/35916259/
- The Role of Fractional Radiofrequency in Long-term Acne Remission and Reduction of Acne Scar Load. PubMed, 2025. https://pubmed.ncbi.nlm.nih.gov/39817790/
- Microneedling in Dermatology: A Comprehensive Review of Applications, Techniques, and Outcomes. PMC, National Center for Biotechnology Information. https://pmc.ncbi.nlm.nih.gov/articles/PMC11499218/
- Microneedling – StatPearls – NCBI Bookshelf, 2022. https://www.ncbi.nlm.nih.gov/books/NBK459344/
- Radiofrequency Microneedling: Technology, Devices, and Indications in the Modern Plastic Surgery Practice. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC11181949/
- Microneedling: Advances and widening horizons. PMC, Indian Dermatology Online Journal, 2016. https://pmc.ncbi.nlm.nih.gov/articles/PMC4976400/
- Evaluation of Microneedling Fractional Radiofrequency Device for Treatment of Acne Scars. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4134659/
- Clinical evaluation of the efficacy of fractional radiofrequency for the treatment and reduction of stretch marks: A prospective study. PubMed, Journal of Cosmetic Dermatology, 2022. https://pubmed.ncbi.nlm.nih.gov/36229028/
- Treatment of Stretch Marks Using a New Formulation Combining Nanofractional Radiofrequency Plus Magnetic Nanofractional Radiofrequency. PMC, 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10264298/
- Adjustable Depth Fractional Radiofrequency Combined With Bipolar Radiofrequency: A Minimally Invasive Combination Treatment for Skin Laxity. PMC, Aesthetic Surgery Journal, 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6460431/
- Clinical and histological evaluation of microneedle fractional radiofrequency treatment on facial fine lines and skin laxity in Koreans. PubMed, 2023. https://pubmed.ncbi.nlm.nih.gov/36718800/
- Single Treatment Protocol With Microneedle Fractional Radiofrequency for Treatment of Body Skin Laxity and Fat Deposits. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC8518615/
- Subcutaneous Radiofrequency Microneedling for the Treatment of Thigh Skin Laxity Caused by Weight Loss: A Case Study. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6624002/
- Comparative study of efficacy and safety of fractional CO2 laser and microneedling fractional radiofrequency (MnRF) in the treatment of striae distensae. IP Indian Journal of Clinical and Experimental Dermatology, 2020. https://ijced.org/archive/volume/6/issue/3/article/7689